
Sciatica vs Piriformis Syndrome: How to Tell the Difference
If you've ever felt a sharp, burning, or electric pain shooting from your lower back or buttock down the back of your leg, you've probably typed "sciatica" into Google. But here's the catch: not all sciatic-type leg pain is actually sciatica. A very similar — and frequently misdiagnosed — condition called piriformis syndrome can produce nearly identical symptoms.
The two conditions are often confused because they share a common feature: irritation of the sciatic nerve. But the root cause, the best treatment approach, and the recovery timeline are quite different. Getting the right diagnosis matters, because treating piriformis syndrome like a disc-related sciatica problem (or vice versa) can slow down your recovery significantly.
At Millwoods Physio, this is one of the most common sources of confusion we see in clients walking through our doors in southeast Edmonton. This guide breaks down exactly how to tell the two apart.
Difference Between Sciatica and Piriformis Syndrome?
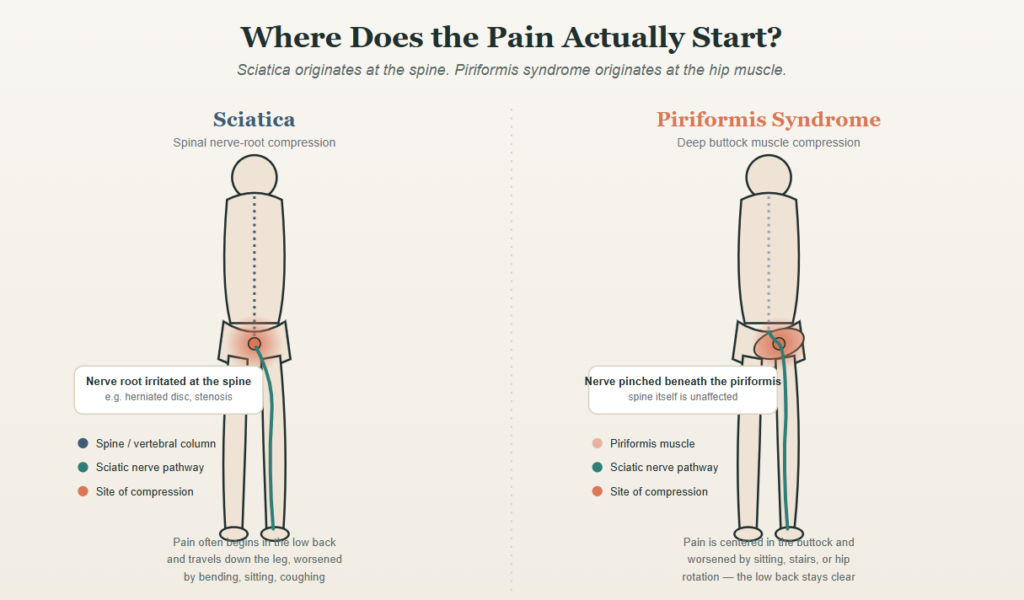
Sciatica is a symptom, not a diagnosis. It refers to nerve pain caused by compression or irritation of the sciatic nerve roots, most commonly from a herniated disc, spinal stenosis, or degenerative changes in the lumbar spine.
Piriformis syndrome is a specific condition where the piriformis muscle — a small muscle deep in the buttock — spasms or tightens and compresses the sciatic nerve as it passes underneath (or, in some people, through) the muscle.
In short: sciatica usually starts in the spine. Piriformis syndrome starts in the hip/buttock muscle. Both can cause sciatic nerve symptoms down the leg, which is why they're so often mixed up.
What Is Sciatica?
Sciatica describes pain that travels along the path of the sciatic nerve — from the lower back, through the buttock, and down the back of the leg, sometimes reaching the foot. It happens when one of the nerve roots that form the sciatic nerve (typically at L4, L5, or S1) gets compressed or inflamed at the spine.
Common Causes of Sciatica
- Herniated or bulging lumbar disc
- Spinal stenosis (narrowing of the spinal canal)
- Degenerative disc disease
- Spondylolisthesis (a vertebra slipping forward)
- Bone spurs pressing on a nerve root
Typical Sciatica Symptoms
- Pain that starts in the low back and radiates down one leg
- Numbness, tingling, or weakness following a specific nerve pattern (often into the calf or foot)
- Pain that worsens with sitting, bending forward, coughing, or sneezing
- Symptoms often affect one side and follow a clear line down the leg
- May include reflex changes or measurable muscle weakness
What Is Piriformis Syndrome?
The piriformis is a small, flat muscle that runs from your sacrum (the base of your spine) to the top of your thighbone, deep underneath your glutes. The sciatic nerve runs directly beneath this muscle in most people. When the piriformis becomes tight, inflamed, or goes into spasm, it can compress or irritate the nerve right at that point — producing pain that feels a lot like spinal sciatica, even though the spine itself is fine.
Common Causes of Piriformis Syndrome
- Prolonged sitting (especially on hard surfaces or with a wallet in the back pocket)
- Overuse from running, cycling, or repetitive hip rotation
- Muscle imbalance or weakness in the glutes and hips
- Direct trauma or a fall onto the buttock
- Sudden increase in activity level or training load
Typical Piriformis Syndrome Symptoms
- Deep, aching pain centered in the buttock, often worse with sitting
- Pain that may radiate down the leg but tends to be less predictable than true nerve-root sciatica
- Tenderness when pressing directly on the piriformis muscle (mid-buttock)
- Pain provoked by hip rotation, crossing the legs, or climbing stairs
- Low back itself is usually not painful or restricted
- No reflex changes (a key differentiator your physiotherapist will check)
Side-by-Side Comparison
| Feature | Sciatica (Spinal Origin) | Piriformis Syndrome |
|---|---|---|
| Primary source | Nerve root compression in the lumbar spine | Muscle compression in the buttock |
| Pain location | Often starts in low back, travels down leg | Centered in buttock, may travel down leg |
| Sitting | Often painful, especially prolonged sitting | Very often the main trigger |
| Back movement | Bending, twisting, coughing aggravate pain | Back movement usually pain-free |
| Hip rotation/stretch | Less specific aggravation | Strongly aggravates symptoms |
| Reflexes | Can be diminished | Usually normal |
| Numbness/weakness | Common, follows nerve pattern | Less common, less defined pattern |
| Imaging findings | May show disc herniation or stenosis | Usually normal spine imaging |
How Physiotherapists Tell Them Apart
Since both conditions can mimic each other, a physiotherapist uses a combination of your history and specific clinical tests rather than relying on symptoms alone.
- Detailed history — When did it start? What movement or position triggers it? Is sitting or spinal movement the bigger problem?
- Lumbar spine assessment — Range of motion, and whether back movements reproduce your leg pain (a strong sign of spinal involvement).
- Neurological screening — Reflexes, muscle strength, and sensation testing to check for nerve root involvement.
- Straight Leg Raise test — More commonly positive in true sciatica from a disc issue.
- Piriformis-specific tests — Such as the FAIR test (Flexion, Adduction, Internal Rotation) and resisted hip external rotation, which reproduce pain when the piriformis is the culprit.
- Palpation — Direct, focused tenderness over the piriformis muscle itself points away from a purely spinal cause.
This is why a proper hands-on assessment matters more than searching symptoms online — the overlap between these two conditions is exactly where self-diagnosis tends to go wrong.
Treatment: Why the Approach Is Different
Because the underlying cause differs, treatment that helps one condition can be ineffective — or even unhelpful — for the other.
For Sciatica (Spinal Origin)
- Directional preference exercises (often extension-based for disc issues)
- Nerve flossing/gliding techniques
- Core and lumbar stabilization
- Postural and ergonomic correction
- Activity modification while inflammation settles
For Piriformis Syndrome
- Piriformis and deep hip rotator stretching
- Soft tissue release/manual therapy to the glutes and hip rotators
- Glute strengthening to reduce compensatory overuse of the piriformis
- Movement retraining (hip hinge mechanics, running or cycling form)
- Activity and sitting posture modification
A physiotherapist builds your plan around which structure is driving your symptoms — which is exactly why getting an accurate diagnosis early shortens your recovery time.
When to See a Physiotherapist Right Away
Most cases of sciatica and piriformis syndrome respond well to conservative physiotherapy treatment. However, seek prompt medical attention if you experience:
- Loss of bladder or bowel control
- Numbness in the groin or inner thighs (saddle anesthesia)
- Progressive leg weakness
- Bilateral leg symptoms
These can indicate a more serious condition called cauda equina syndrome, which requires emergency care.
Frequently Asked Questions
Can you have sciatica and piriformis syndrome at the same time?
Yes. In some cases, a tight piriformis develops as a compensation pattern alongside an existing spinal issue, or chronic poor movement mechanics contribute to both. A physiotherapist can identify whether one or both structures are contributing to your symptoms.
Does piriformis syndrome show up on an MRI?
Not reliably. Standard imaging is designed to assess the spine, discs, and bones — it typically won't show piriformis muscle tightness or spasm. This is one reason piriformis syndrome is frequently missed or misdiagnosed when imaging comes back "normal."
How long does it take to recover from piriformis syndrome vs. sciatica?
Piriformis syndrome often improves within 2–6 weeks with targeted stretching, soft tissue work, and strengthening. Sciatica from a disc issue can take longer — typically 6–12 weeks — depending on severity, though many people see meaningful improvement within the first few weeks of treatment.
What's the fastest way to relieve piriformis pain at home?
Gentle piriformis stretches (such as a seated figure-4 stretch), avoiding prolonged sitting, and alternating ice/heat can help in the short term. However, addressing the underlying cause — usually hip weakness or movement compensation — is what prevents it from coming back.
Should I stretch if I have sciatica?
It depends on the cause, which is exactly why self-treating can backfire. Some stretches that help piriformis syndrome can aggravate a disc-related sciatica, and vice versa. A proper assessment tells you which movements help and which to avoid.
Get an Accurate Diagnosis at Millwoods Physio
Sciatic nerve pain is frustrating to live with, and guessing at the cause often leads to wasted time on the wrong exercises. Our physiotherapists in Millwoods, Edmonton perform a thorough assessment to pinpoint whether your symptoms are coming from your spine, your piriformis muscle, or a combination of both — then build a treatment plan specific to your cause.
Don't keep guessing why your leg pain won't go away. Book an assessment with Millwoods Physio today and get a clear answer, along with a recovery plan built around it.








